Parkinson’s disease (also known as Parkinson disease or Parkinson’s Disease) is a degenerative disorder of the central nervous system that often impairs the sufferer’s motor skills and speech.
History of Parkinson’s Disease
Symptoms of Parkinson’s disease have been known and treated since ancient times. However, it was not formally recognized and its symptoms were not documented until 1817, in An Essay on the Shaking Palsy. by the British physician James Parkinson. Parkinson’s disease was then known as paralysis agitans, the term “Parkinson’s disease” being coined later by Jean Martin Charcot. The underlying biochemical changes in the brain were identified in the 1950’s, due largely to the work of Swedish scientist Arwid Carlsson, who later went on to win a Nobel prize.
What is Parkinson’s Disease?
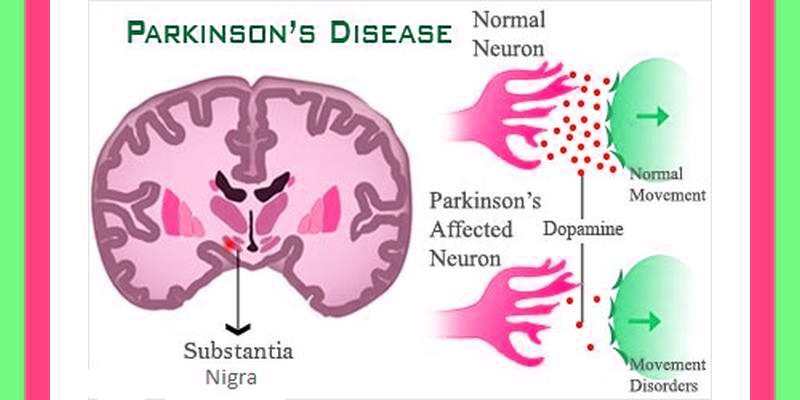
Parkinson’s disease is a disorder that affects nerve cells, or neurons, in a part of the brain that controls muscle movement. In Parkinson’s, neurons that make a chemical called dopamine die or do not work properly. Dopamine normally sends signals that help coordinate your movements. Parkinson’s is a disease that causes a progressive loss of nerve cell function in the part of the brain that controls muscle movement. Progressive means that this disease’s effects get worse over time.
Symptoms of Parkinson’s Disease
Parkinson’s disease belongs to a group of conditions called movement disorders. The primary symptoms are the results of decreased stimulation of the motor cortex by the basal ganglia, normally caused by the insufficient formation and action of dopamine ,which is produced in the dopaminergic neurons of the brain. Secondary symptoms may include high level cognitive dysfunction and subtle language problems. Parkinson’s Disease is both chronic and progressive.
Early symptoms of Parkinson’s Disease are subtle and occur gradually. Affected people may feel mild tremors or have difficulty getting out of a chair. They may notice that they speak too softly or that their handwriting is slow and looks cramped or small. They may lose track of a word or thought, or they may feel tired, irritable, or depressed for no apparent reason. This very early period may last a long time before the more classic and obvious symptoms appear.
Friends or family members may be the first to notice changes in someone with early Parkinson’s Disease. They may see that the person’s face lacks expression and animation (known as “masked face”) or that the person does not move an arm or leg normally. They also may notice that the person seems stiff, unsteady, or unusually slow.
As the disease progresses, the shaking or tremor that affects the majority of Parkinson’s patients may begin to interfere with daily activities. Patients may not be able to hold utensils steady or they may find that the shaking makes reading a newspaper difficult. Tremor is usually the symptom that causes people to seek medical help.
People with Parkinson’s Disease often develop a so-called Parkinsonian gait that includes a tendency to lean forward, small quick steps as if hurrying forward (called festination), and reduced swinging of the arms. They also may have trouble initiating movement (start hesitation), and they may stop suddenly as they walk (freezing).
Parkinson’s Disease does not affect everyone the same way, and the rate of progression differs among patients. Tremor is the major symptom for some patients, while for others; tremor is nonexistent or very minor.
Parkinson’s Disease symptoms often begin on one side of the body. However, as it progresses, the disease eventually affects both sides. Even after the disease involves both sides of the body, the symptoms are often less severe on one side than on the other.
The four primary symptoms of Parkinson’s Disease are:
- Tremor. The tremor associated with Parkinson’s Disease has a characteristic appearance. Typically, the tremor takes the form of a rhythmic back-and-forth motion at a rate of 4-6 beats per second. It may involve the thumb and forefinger and appear as a “pill rolling” tremor. Tremor often begins in a hand, although sometimes a foot or the jaw is affected first. It is most obvious when the hand is at rest or when a person is under stress. For example, the shaking may become more pronounced a few seconds after the hands are rested on a table. Tremor usually disappears during sleep or improves with intentional movement.
- Rigidity–. Rigidity, or a resistance to movement, affects most people with Parkinson’s Disease. A major principle of body movement is that all muscles have an opposing muscle. Movement is possible not just because one muscle becomes more active, but because the opposing muscle relaxes. In Parkinson’s Disease, rigidity comes about when, in response to signals from the brain, the delicate balance of opposing muscles is disturbed. The muscles remain constantly tensed and contracted so that the person aches or feels stiff or weak. The rigidity becomes obvious when another person tries to move the patient’s arm, which will move only in ratchet-like or short, jerky movements known as “cogwheel” rigidity.
- Bradykinesia. – Bradykinesia, or the slowing down and loss of spontaneous and automatic movement, is particularly frustrating because it may make simple tasks somewhat difficult. The person cannot rapidly perform routine movements. Activities once performed quickly and easily — such as washing or dressing — may take several hours.
- Postural instability.- Postural instability, or impaired balance, causes patients to fall easily. Affected people also may develop a stooped posture in which the head is bowed and the shoulders are drooped.
A number of other symptoms may accompany Parkinson’s Disease. Some are minor; others are not. Many can be treated with medication or physical therapy. No one can predict which symptoms will affect an individual patient, and the intensity of the symptoms varies from person to person.
- Depression –This is a common problem and may appear early in the course of the disease, even before other symptoms are noticed. Fortunately, depression usually can be successfully treated with antidepressant medications. Hallucinations,delusions and paranoia may develop.
- Emotional changes –Some people with Parkinson’s Disease become fearful and insecure. Perhaps they fear they cannot cope with new situations. They may not want to travel, go to parties, or socialize with friends. Some lose their motivation and become dependent on family members. Others may become irritable or uncharacteristically pessimistic.
- Difficulty with swallowing and chewing- Muscles used in swallowing may work less efficiently in later stages of the disease. In these cases, food and saliva may collect in the mouth and back of the throat, which can result in choking or drooling. These problems also may make it difficult to get adequate nutrition. Speech-language therapists, occupational therapists, and dieticians can often help with these problems.
- Speech changes- About half of all Parkinson’s Disease patients have problems with speech. They may speak too softly or in a monotone, hesitate before speaking, slur or repeat their words, or speak too fast. A speech therapist may be able to help patients reduce some of these problems.
- Urinary problems or constipation- In some patients, bladder and bowel problems can occur due to the improper functioning of the autonomic nervous system, which is responsible for regulating smooth muscle activity. Some people may become incontinent, while others have trouble urinating. In others, constipation may occur because the intestinal tract operates more slowly. Constipation can also be caused by inactivity, eating a poor diet, or drinking too little fluid. The medications used to treat Parkinson’s Disease also can contribute to constipation. It can be a persistent problem and, in rare cases, can be serious enough to require hospitalization.
- Skin problems- In Parkinson’s Disease, it is common for the skin on the face to become very oily, particularly on the forehead and at the sides of the nose. The scalp may become oily too, resulting in dandruff. In other cases, the skin can become very dry. These problems are also the result of an improperly functioning autonomic nervous system. Standard treatments for skin problems can help. Excessive sweating, another common symptom, is usually controllable with medications used for Parkinson’s Disease.
- Sleep problems- Sleep problems common in Parkinson’s Disease include difficulty staying asleep at night, restless sleep, nightmares and emotional dreams, and drowsiness or sudden sleep onset during the day. Patients with Parkinson’s Disease should never take over-the-counter sleep aids without consulting their physicians.
- Dementia or other cognitive problems- Some, but not all, people with Parkinson’s Disease may develop memory problems and slow thinking. In some of these cases, cognitive problems become more severe, leading to a condition called Parkinson’s dementia late in the course of the disease. This dementia may affect memory, social judgment, language, reasoning, or other mental skills.
- Orthostatic hypotension- Orthostatic hypotension is a sudden drop in blood pressure when a person stands up from a lying-down position. This may cause dizziness, lightheadedness, and, in extreme cases, loss of balance or fainting. Studies have suggested that, in Parkinson’s Disease, this problem results from a loss of nerve endings in the sympathetic nervous system that controls heart rate, blood pressure, and other automatic functions in the body. The medications used to treat Parkinson’s Disease also may contribute to this symptom.
- Muscle cramps and dystonia- The rigidity and lack of normal movement associated with Parkinson’s Disease often causes muscle cramps, especially in the legs and toes. Massage, stretching, and applying heat may help with these cramps. Parkinson’s Disease also can be associated with dystonia — sustained muscle contractions that cause forced or twisted positions. Dystonia in Parkinson’s Disease is often caused by fluctuations in the body’s level of dopamine. It can usually be relieved or reduced by adjusting the person’s medications.
- Pain- Many people with Parkinson’s Disease develop aching muscles and joints because of the rigidity and abnormal postures often associated with the disease. Certain exercises also may help. People with Parkinson’s Disease also may develop pain due to compression of nerve roots or dystonia-related muscle spasms. In rare cases, people with Parkinson’s Disease may develop unexplained burning, stabbing sensations. This type of pain, called “central pain,” originates in the brain. Dopaminergic drugs, opiates, antidepressants, and other types of drugs may all be used to treat this type of pain.
- Fatigue and loss of energy- The unusual demands of living with Parkinson’s Disease often lead to problems with fatigue, especially late in the day. Fatigue may be associated with depression or sleep disorders, but it also may result from muscle stress or from overdoing activity when the person feels well. Fatigue also may result fromakinesia – trouble initiating or carrying out movement. Exercise, good sleep habits, staying mentally active, and not forcing too many activities in a short time may help to alleviate fatigue.
- Sexual dysfunction- Parkinson’s Disease often causes erectile dysfunction because of its effects on nerve signals from the brain or because of poor blood circulation. Parkinson’s Disease-related depression or use of antidepressant medication also may cause decreased sex drive and other problems. These problems are often treatable.
- Sensation disturbances- Impaired visual contrast sensitivity , spatial reasoning, colour discrimination, convergence insufficiency (characterized by double vision ) and oculomotor disturbances.
- Dizziness and fainting; usually attributable to orthostatic hypotension, a failure of the autonomous nervous system to adjust blood pressure in response to changes in body position
- Impaired perception (the awareness of bodily position in three-dimensional space)
- Reduction or loss of sense of smell (microsmia or anosmia) – can occur years prior to diagnosis,
- Pain: neuropathic, muscle, joints and tendons, attributable to tension, dystonia, rigidity, joint stiffness, and injuries associated with attempts at accommodation
Cause of Parkinson’s Disease
The main causes could be graded under four headings:
- Genetic
- Toxins
- Head injury
- Drug induced
Parkinson’s disease occurs when nerve cells, or neurons, in an area of the brain known as the substantia nigra die or become impaired. Normally, these neurons produce an important brain chemical known as dopamine. Dopamine is a chemical messenger responsible for transmitting signals between the substantia nigra and the next “relay station” of the brain, the corpus striatum, to produce smooth, purposeful movement. Loss of dopamine results in abnormal nerve firing patterns within the brain that cause impaired movement. Studies have shown that most Parkinson’s patients have lost 60 to 80 percent or more of the dopamine-producing cells in the substantia nigra by the time symptoms appear. Recent studies have shown that people with Parkinson’s Disease also have loss of the nerve endings that produce the neurotransmitter nor epinephrine. Nor epinephrine, which is closely related to dopamine, is the main chemical messenger of the sympathetic nervous system, the part of the nervous system that controls many automatic functions of the body, such as pulse and blood pressure. The loss of nor epinephrine might help explain several of the non-motor features seen in Parkinson’s Disease, including fatigue and abnormalities of blood pressure regulation.
- Genetic causes- Scientists have identified several genetic mutations associated with Parkinson’s Disease, and many more genes have been tentatively linked to the disorder. Studying the genes responsible for inherited cases of Parkinson’s Disease can help researchers understand both inherited and sporadic cases. The same genes and proteins that are altered in inherited cases may also be altered in sporadic cases by environmental toxins or other factors.
- Environmental toxins –Although the importance of genetics in Parkinson’s Disease is increasingly recognized, most researchers believe environmental exposures increase a person’s risk of developing the disease. Even in familial cases, exposure to toxins or other environmental factors may influence when symptoms of the disease appear or how the disease progresses. There are a number of toxins, such as 1-methyl-4-phenyl-1, 2, 3, 6-tetrahydropyridine, or MPTP (found in some kinds of synthetic heroin), that can cause Parkinson Ian symptoms in humans. Other, still-unidentified environmental factors also may cause Parkinson’s Disease in genetically susceptible individuals.
- Viruses are another possible environmental trigger for Parkinson’s Disease. People who developed encephalopathy after a 1918 influenza epidemic were later stricken with severe, progressive Parkinson’s-like symptoms. A group of Taiwanese women developed similar symptoms after contracting herpes virus infections. In these women, the symptoms, which later disappeared, were linked to a temporary inflammation of the substantia nigra.
- Several lines of research suggest that mitochondria may play a role in the development of Parkinson’s Disease. Mitochondria are the energy-producing components of the cell and are major sources of free radicals — molecules that damage membranes, proteins, DNA, and other parts of the cell. This damage is often referred to as oxidative stress. Oxidative stress-related changes, including free radical damage to DNA, proteins, and fats, have been detected in brains of Parkinson’s Disease patients.
- Other research suggests that the cell’s protein disposal system may fail in people with Parkinson’s Disease, causing proteins to build up to harmful levels and trigger cell death. Additional studies have found evidence that clumps of protein that develop inside brain cells of people with Parkinson’s Disease may contribute to the death of neurons, and that inflammation or over stimulation of cells (because of toxins or other factors) may play a role in the disease. However, the precise role of the protein deposits remains unknown. Some researchers even speculate that the protein buildup is part of an unsuccessful attempt to protect the cell. While mitochondrial dysfunction, oxidative stress, inflammation, and many other cellular processes may contribute to Parkinson’s Disease, the actual cause of the dopamine cell death is still undetermined.
Parkinson’s Disease Diagnosis
A doctor may diagnose a person with Parkinson’s disease based on the patient’s symptoms, neurological examinations and medical history. No blood tests or x-rays can show whether a person has Parkinson’s disease. However, some kinds of x-rays can help the doctor make sure nothing else is causing symptoms. If symptoms go away or get better when the person takes a medicine called levodopa, it’s fairly certain that he or she has Parkinson’s disease.
The disease can be difficult to diagnose accurately. The Unified disease rating scale is the primary clinical tool used to assist in diagnosis and determine severity of Parkinson’s Disease. Indeed, only 75% of clinical diagnoses of Parkinson’s Disease are confirmed at autopsy. Early signs and symptoms of Parkinson’s Disease may sometimes be dismissed as the effects of normal aging. The physician may need to observe the person for some time until it is apparent that the symptoms are consistently present. Usually doctors look for shuffling of feet and lack of swing in the arms. Doctors may sometimes request brain scans or laboratory tests in order to rule out other diseases. However, CT and MRI brain scans of people with Parkinson’s Disease usually appear normal.
The Unified Parkinson’s Disease Rating Scale (UParkinson’s DiseaseRS) is a rating scale used to follow the longitudinal course of Parkinson’s disease. It is made up of the following sections:
- Mentation, behavior, and mood;
- Activities of daily living;
- Motor;
- Complications of therapy;
- Hoehn and Yahr Stage;
Hoehn and Yahr Staging of Parkinson’s Disease
- Stage one Symptoms on one side of the body only.
- Stage two Symptoms on both sides of the body. No impairment of balance.
- Stage three Balance impairment. Mild to moderate disease. Physically independent.
- Stage four Severe disability, but still able to walk or stand unassisted.
- Stage five Wheelchair-bound or bedridden unless assisted.
Prognosis of Parkinson’s disease
Parkinson’s Disease is not by itself a fatal disease, but it does get worse with time. The average life expectancy of a Parkinson’s Disease patient is generally the same as for people who do not have the disease. However, in the late stages of the disease, Parkinson’s Disease may cause complications such as choking, pneumonia, and falls that can lead to death. Fortunately, there are many treatment options available for people with Parkinson’s Disease.
The progression of symptoms in Parkinson’s Disease may take 20 years or more. In some people, however, the disease progresses more quickly. There is no way to predict what course the disease will take for an individual person.
Treatment of Parkinson’s Disease
Allopathic treatment–
There is no cure for Parkinson’s disease. But medicines can help control the symptoms of the disease. Some of the medicines used to treat Parkinson’s disease include carbidopa-levodopa (one brand name: Sinemet), bromocriptine (brand name: Parlodel), selegiline (one brand name: Eldepryl), pramipexole (brand name: Mirapex), ropinirole (brand name: Requip), and tolcapone (brand name: Tasmar).
Side effects of drugs used for Parkinson’s disease
The most common drugs used in the treatment are:L-dopa – It is the most widely used drug but also causes many side effects because only 1-5% of L-dopa enters dopaminergic neurons rest is metabolized to dopamine elsewhere.
Initially it causes complaints like:
Nausea
Vomiting
Reduced blood pressure
Restlessness
Drowsiness and sudden sleepLater it can complicate the condition even further and can cause:
Hallucinations
PsychosisYounger patients of Parkinson’s suffer more from its side effects as:
Dyskinesis
Painful ‘off’ dystonias
Tremors intensified
Dyskinesias, or involuntary movements such as twitching, twisting, and writhing, commonly develop in people who take large doses of levodopa over an extended period. These movements may be either mild or severe and either very rapid or very slow. The dose of levodopa is often reduced in order to lessen these drug-induced movements.
However, the Parkinson’s Disease symptoms often reappear even with lower doses of medication. Doctors and patients must work together closely to find a tolerable balance between the drug’s benefits and side effects.The period of effectiveness after each dose may begin to shorten, called the wearing-off effect. Another potential problem is referred to as the on-off effect — sudden, unpredictable changes in movement, from normal to Parkinson Ian movement and back again. These effects probably indicate that the patient’s response to the drug is changing or that the disease is progressing
Dopamine agonists – side effects includes
Somnolence
Hallucinations
Insomnia
Oedema
Less motor fluctuations
Dyskinesis (twisting / turning) movementsIn rare cases, they can cause compulsive behavior, such as an uncontrollable desire togamble, hyper sexuality, or compulsive shopping. Bromocriptine can also causefibrosis, or a buildup of fibrous tissue, in the heart valves or the chest cavity. Fibrosis usually goes away once the drugs are stopped.
MAO-B inhibitors. These drugs inhibit the enzyme monoamine oxidase B, or MAO-B, which breaks down dopamine in the brain. MAO-B inhibitors cause dopamine to accumulate in surviving nerve cells and reduce the symptoms of Parkinson’s Disease. Selegiline, also called deprenyl, is an MAO-B inhibitor that is commonly used to treat Parkinson’s Disease. Studies supported by the NINDS have shown that selegiline can delay the need for levodopa therapy by up to a year or more. When selegiline is given with levodopa, it appears to enhance and prolong the response to levodopa and thus may reduce wearing-off fluctuations.
Selegiline is usually well-tolerated, although side effects may include
Nausea
Orthostatic hypotension,
Stomatitis
Insomnia. It should not be taken with the antidepressant fluoxetine or the sedative mepiridine, because combining seligiline with these drugs can be harmful.
COMT inhibitors. COMT stands for catechol-O-methyltransferase, another enzyme that helps to break down dopamine. Two COMT inhibitors are approved to treat Parkinson’s Disease in the United States: entacapone and tolcapone. These drugs prolong the effects of levodopa by preventing the breakdown of dopamine. COMT inhibitors can decrease the duration of “off” periods, and they usually make it possible to reduce the person’s dose of levodopa.
The most common side effect is diarrhea. The drugs may also cause nausea, sleep disturbances, dizziness, urine discoloration, abdominal pain, low blood pressure, or hallucinations.
Anticholinergics. These drugs, which include trihexyphenidyl, benztropine, and ethopropazine, decrease the activity of the neurotransmitter acetylcholine and help to reduce tremors and muscle rigidity. Only about half the patients who receive anticholinergics are helped by it, usually for a brief period and with only a 30 percent improvement. Side effects may include dry mouth, constipation, urinary retention, hallucinations, memory loss, blurred vision, and confusion.
Homeopathy Treatment & Homeopathic Remedies for Parkinson’s Disease
Homeopathy treats the person as a whole. It means that homeopathic treatment focuses on the patient as a person, as well as his pathological condition. The homeopathic medicines are selected after a full individualizing examination and case-analysis, which includes the medical history of the patient, physical and mental constitution etc. A miasmatic tendency (predisposition/susceptability) is also often taken into account for the treatment of chronic conditions. The medicines given below indicate the therapeutic affinity but this is not a complete and definite guide to the treatment of this condition. The symptoms listed against each medicine may not be directly related to this disease because in homeopathy general symptoms and constitutional indications are also taken into account for selecting a remedy. To study any of the following remedies in more detail, please visit our Materia Medica section. None of these medicines should be taken without professional advice.Reportorial rubric:
Murphy: Diseases: Paralysis-agitans.
Clarke: Paralysis agitans.
Boericke: Nervous system: Paralysis-Type – agitans
Homeopathic Remedies
- Mercurius
- Zincum-Metallicum
- Rhus-tox
- Aurum met
- Nux vomica
- Gelsemium
- Argentum Nitricum
- Agaricus Muscarius
- Cocculus
- Lathyrus
- Physostigma
- Ambra Grisea
- Heloderma
- Mag-phos
- Bufo Rana
- Rhus tox
- Zincum met
- Tarentula
- Plumbum Metalicum
- Conium
Mercurius
Weakness of limbs, trembling of extremities, especially hands. Paralytic agitans. Lacerating pain in joints. Cold and clammy sweat on limbs. Oily perspiration.Tremors everywhere in body. Weakness with trembling from least exertion. All symptoms are aggravated at night, warmth of bed, Damp, cold, rainy weather and during perspiration. Complaints increase during sweating and rest. All symptoms always associated with weariness, prostration and trembling.
Slow in answering questions. Memory weakened and loss of will power. Skin alwaysmoist and freely perspiring. Itching worse warmth of bed
Zincum-Metallicum
Violent trembling (twitching) of the whole body especially after emotions. Twitching in children. Chorea. Paralysis of hands and feet. Trembling of hands while writing. Lameness, weakness, trembling and twitching of various muscles. Feet in continued motion, cannot keep still. Worse touch, between 5-7 pm., after dinner, better eating, discharges.
Rhus-tox
When the tremors start with pain which is relieved by motion. There is stiffness of the parts affected. Numbness and formication, after overwork and exposure. Paralysis; trembling after exertion. Limbs stiff and paralysed.All joints hot and painful. Crawling and tingling sensation in the tips of fingers. Worse during sleep, cold, wet rainy weather and after rain, night, during rest, drenching and when lying on back or right side. Better warm, dry weather, motion, walking, change of position, rubbing, stretching out limbs.
Gelsemium
Centers its action on nervous system, causing various degrees of motor paralysis…Dizziness, drowsiness, dullness and trembling are the hallmark of this remedy. Trembling ranks the highest in this remedy, weakness and paralysis, especially of the muscles of the head. Paralysis of various groups of muscles like eyes, throat, chest, sphincters and extremities. Head remedy for tremors. Mind sluggish and muscular system relaxed. Staggering gait. Loss of power of muscular control. Cramps in muscles of forearm. Excessive trembling and weakness of all limbs. Worse by dampness, excitement, bad news. Better by bending forwards, profuse urination, continued motion and open air.
Argentum Nitricum
It is complimentary to Gelsemium. Memory impaired; easily excited and angered; flatulence and greenish diarrhea.Inco-ordination, loss of control and imbalance with trembling and general debility. Paralysis with mental and abdominal symptoms. Rigidity of calves. Walks and stands unsteadily. Numbness of body. Specially arms.
Agaricus Muscarius
Trembling, itching and jerking, stiffness of muscles; itching of skin over the affected parts and extreme sensitiveness of the spine. Cannot bear touch. Jerking and trembling are strong indications. Chorea and twitching ceases during sleep. Paralysis of lower limbs with spasmodic conditions of arms. Numbness of legs on crossing them. Paralytic pain in left arm followed by palpitation. Stiffness all over with pain over hips.
Cocculus
Head trembles while eating and when it is raised higher. Knees sink down from weakness. Totters while walking with tendency to fall on one side. Cracking of the knee when moving. Lameness worse by bending. Trembling and pain in limbs. One-sided paralysis worse after sleep. Intensely painful, paralytic drawing. Limbs straightened out and painful when flexed.
It shows special affinity for light haired females especially during pregnancy.
Lathyrus
Tremors of the upper extremities with paralytic weakness of the lower limbs. Feels as if limbs are hard and contracted; limbs feel heavy. Feels as if floor is irregular and is obliged to keep his eyes on the ground to guide his feet. Affects the lateral and anterior columns of cord. Does not produce pain. Reflexes always increased. Lateral sclerosis and Infantile paralysis. Finger tips numb. Tremulous, tottering gait. Excessive rigidity of legs with spastic gait. Knees knock against each other while walking. Cannot extend or cross legs when siting.Stiff and lame ankles.
Physostigma
Marked fibrillary tremors and spasms of the muscles, worse from motion or application of cold water. Palpitation and fluttering of the heart felt throughout the body. Depresses the motor and reflex activity of the cord and causes the loss of sensibility to pain, muscle weakness and paralysis. Paralysis and tremors, chorea. Meningeal irritation with rigidity of muscles. Pain in right popliteal space. Burning and tingling in spine. Hands and feet numb with sudden jerking of limbs on going to sleep. Crampy pain in limbs.
Ambra Grisea
Tremors with numbness, limbs go to sleep on the slightest movement, coldness and stiffness of limbs. The finger nails become brittle and are shriveled. Cramps in hands and fingers. Worse grasping anything. Cramps in legs. Extreme nervous hypersensitiveness. Dread of people and desire to be alone. Music causes weeping. One sided complains call for it.
Heloderma
Trembling along nerves in limbs. Tired feeling, very weak and nervous, fainting, numb sensation. It causes locomotor ataxia. The eyes become more prominent and corneal opacities visible. Very depressed and sensation as if would fall on right side. Sensationas if walking on sponge. As if the feet were swollen. When walking, lifts feet higher than usual and puts down heel hard. Stretching relieves pains in muscles and limbs.
Mag-phos
Trembling; shaking of hands, involuntary. Paralysis agitans. Cramps in calves, feet very tender. Twitching, Chorea, cramps. Numbness of finger tips. Worse right side, cold, touch, night. Better warmth, bending double, pressure and friction.
Bufo Rana
Special action on nervous system. Painful paralysis. Pain in loins, numbness and cramps. Staggering gait. Feels as if a peg is driven into joints. Worse—Warm room. Better bathing or cold air. Putting feet in cold water.
Tarentula
Remarkable nervous phenomena. Chorea, extreme restlessness and Paralysis agitans. Must keep in constant motion even though walking aggravates. Numbness of legs with twitching and jerking. Extraordinary contractions and movements.
Plumbum Metalicum
Paralytic agitans. Paralysis of single muscles. Cannot raise or lift anything. Extension is difficult. Paralysis from over-exertion of extensor muscles in piano players. Wrist drop. Loss of patellar reflex. Pain in right big toe at night. Hands and feet cold. Infantile paralysis and neuritis.
Conium
Heavy, weary and paralyzed limbs. Trembling and unsteady hands. Muscular weakness especially of lower extremities. Perspiration of hands. Putting feet on chair relieves.Ascending paralysis ending in death by failure of respiration. Worse by lying down, turning or rising in bed, cold, exertion. Better by darkness, limbs hanging down, motion, pressure.



(PARKINSON’S DISEASE CURED)
I am a 77-year-old lady. My Parkinson’s disease appeared at the age of 74, with no hope of a cure from the hospital i looked further for an alternative treatments, a friend of mine told me about NewLife Herbal Clinic in Johannesburg South Africa who sell herbal treatments for diseases including parkinson’s disease, I contacted the herbal clinic via their website and purchased the parkinson’s herbal remedy. I received the herbal remedy through Fastlink couriers within 8 days and i immediately commenced usage as prescribed, i used the herbal remedy for about a month and 1 week, my condition has greatly improved, all my symptoms including tremor in both hands, shaking, rigid muscle dissapeared, I am PD free! contact NewLife Herbal Clinic via their email newlifeherbalclinic(at)gmail(dot)com. PD is not a death sentence, there is a cure! (Please write email in right format)
thank you for sharing that info, do you perhaps have a phone number and contact name, regards
Bonjour Madam; Ja mogu vam pisat’ na russkom? Boleju Parcinsonom s 50 let Ochen’ zainteresovalsja vashey podskazkoy Proshu vas opisat’ podrobnee Merci
Hi katie, i also used this herbal formula and it really helped me
My wife was diagnosed of Parkinsons Disease at age 59. She had severe calf pain, muscle pain, tremors, slurred speech, frequent falls, loss of balance, difficulty in getting up from sitting position. She was put on Senemet for 6 months and then Siferol was introduced and replaced the Senemet. During this time span she was also diagnosed with dementia. She started having hallucinations, lost touch with reality.
This year, our family doctor started her on NewLife Clinic Parkinsons Disease Herbal mixture, 1 month into treatment she improved dramatically. At the end of the full treatment course, the disease is totally under control. No case of dementia, hallucination, weakness, muscle pain or tremors.
Visit NewLife Clinic website ww w.newlifeherbalclinic .com. She is strong again and able to go about daily activities.
David Craven
Lookslike an advert for New Life Herbal Clinic, and nothing to do with Homeopathy!